 English
English عربى
عربى Español
Español русский
русский 中文简体
中文简体






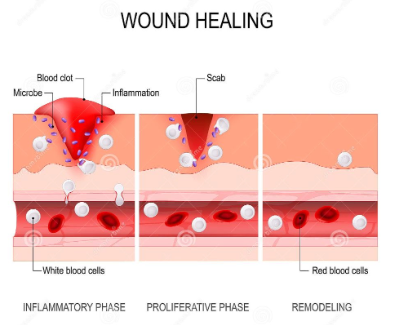
The granulation phase of wound healing signifies the near end of the inflammatory stage, with bright red or pink granular new tissue appearing on the wound surface. Granulation tissue, composed of newly formed capillaries, fibroblasts, and matrix components, marks the transition of a wound from clean to closed. This stage typically occurs between day 3 and day 14 post-injury, with the exact timing depending on wound size, depth, and the patient's overall condition. Many patients, upon seeing red granulation tissue, immediately assume the wound is healed and can relax their care. However, the granulation phase is a critical window determining healing quality and scar appearance. Proper management during this stage directly impacts subsequent epithelial migration and the final smoothness of the scar.
What are the characteristics of normal granulation tissue growth?
Healthy granulation tissue is bright red or coral red, moist and glossy, with a uniform texture. It bleeds easily upon touch, but the bleeding is minimal, and it fills the wound defect at a rate of approximately 1 millimeter per day. If the granulation tissue becomes pale, edematous, brittle, or its growth rate stagnates for more than a week, it usually indicates persistent infection, insufficient local blood supply, or poor systemic nutrition. If the granulation tissue grows excessively, extending beyond the wound edge and forming edematous granulation tissue that protrudes above the surrounding skin, it is medically termed granulation hyperplasia or granulation edema. This condition requires intervention with silver nitrate cauterization or surgical trimming, as it hinders the epidermis from spreading from the edges to the center.
What details should be paid attention to when changing dressings?
During the granulation tissue growth period, the core principle of dressing changes is to protect the newly formed tissue from secondary damage. The choice of dressing should shift from primarily anti-inflammatory and drainage-oriented types to moisturizing and non-adhesive types. When ordinary dry gauze comes into contact with moist granulation tissue, the dried exudate can cause fibers to become embedded in the granulation tissue gaps. Tearing the dressing during changes can directly tear newly formed capillaries and fibroblasts, exposing fresh wounds. Repeated applications will cause the granulation tissue to become pale and sparse. Clinically, it is recommended to use a silicone gel contact layer foam dressing , covering the area before using an outer gauze to absorb excess exudate. Each dressing change should be done gently, moistening any adhesions with saline solution before slowly peeling off the dressing; direct pulling is prohibited. Simultaneously, the color of the exudate should be observed. Normal exudate during the granulation tissue growth period should be pale yellow or clear. If it turns yellowish-green or is accompanied by bloody exudate, it indicates possible infection or damage to the granulation tissue.
What can patients do on their own to help granulation tissue grow?
In terms of diet, the intake of protein and vitamin C directly affects the rate at which fibroblasts synthesize collagen. The recommended daily protein intake is 1.2 to 1.5 grams per kilogram of body weight. A 60-kilogram patient would need 72 to 90 grams of protein daily, roughly equivalent to two eggs, 150 grams of lean meat, and a cup of milk. Vitamin C participates in the cross-linking of collagen molecules; a deficiency reduces the stability of newly formed collagen, making granulation tissue brittle and fragile. Fresh vegetables and fruits are the main sources of vitamin C, with a recommended daily intake of around 200 milligrams. Furthermore, smokers must strictly quit smoking, as nicotine in tobacco causes continuous vasoconstriction, significantly reducing blood supply to granulation tissue. If the wound is located on the lower limb, elevating the affected limb while lying flat can promote venous return and reduce local edema. Controlling underlying diseases also plays a crucial role at this stage. Diabetic patients need to control their fasting blood glucose below 8 mmol/L; persistently high blood glucose inhibits fibroblast proliferation and collagen synthesis, reducing granulation tissue growth by more than half. When blood sugar is high, the chemotaxis and phagocytic function of neutrophils are also inhibited, the risk of infection increases, and granulation tissue is prone to degeneration.
What's the next step after granulation tissue has completely covered the wound?
When granulation tissue fills the defect and becomes flush with the surrounding skin, healing enters the epithelialization stage. At this time, the frequency of dressing changes should be reduced to avoid frequent tearing that could interfere with epidermal cell migration. The wound should be kept moist but not wet. Some dressings can be used for several days without changing; however, this should be done according to your doctor's instructions. If the granulation period has exceeded three weeks without significant progress, or if the wound color turns dark red or even grayish-white, this indicates stagnant healing, and a follow-up visit is necessary for the doctor to reassess the necessity of debridement and the overall systemic support plan. For more information on Innomed® Silicone Foam Dressing Bordered, refer to the Previous Articles. If you have customized needs, you are welcome to contact us; You Wholeheartedly. At long-term medical, we transform this data by innovating and developing products that make life easier for those who need loving care.
Editor: kiki Jia


