 English
English عربى
عربى Español
Español русский
русский 中文简体
中文简体






When changing dressings and smelling a foul odor from a wound, many people's first reaction is that it's infected and they need to immediately use antibiotics or strong disinfectants. This judgment is sometimes correct, but sometimes wrong. A foul-smelling wound is indeed common in infections, especially anaerobic bacterial infections, which have a very distinctive putrid or fecal odor. However, besides infection, there are several other conditions that can also cause an unpleasant odor from a wound, and these do not require antibiotic treatment; using antibiotics in the wrong context can actually slow down healing.
What does an infectious odor look like?
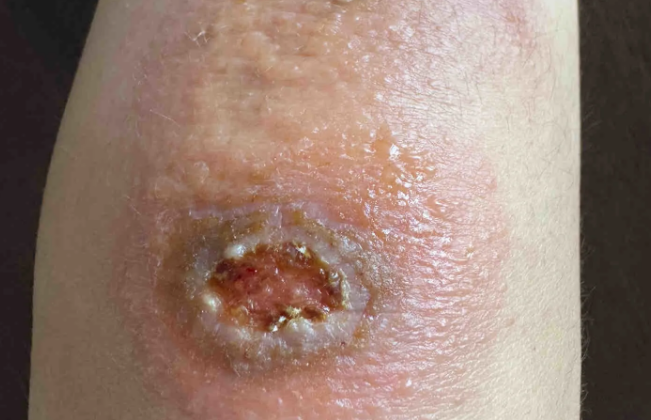
The odor caused by infection has its own characteristics. Anaerobic bacterial infections are the most typical, producing a putrid, rotting, or even fecal smell. These bacteria thrive in anaerobic environments and are most commonly found in deep sinus tracts, under eschars, or on wounds with remaining necrotic tissue. Besides odor, infection is usually accompanied by other symptoms: the wound base changes color from normal red or pink to grayish-white, yellowish-green, or dark purple; the exudate changes from clear pale yellow to cloudy, purulent, and sometimes bloody; the surrounding skin is red, swollen, warm, and tender; the patient may also experience low-grade fever or general weakness. If these symptoms are present simultaneously, the odor is most likely caused by an infection and requires anti-infective treatment.
What are the sources of non-infectious odors?
A foul-smelling wound doesn't always indicate a bacterial infection. The most common cause is the decomposition of necrotic tissue. The black eschar, yellowish-white fascia, or fatty tissue in the wound—these necrotic tissues themselves are inactive and don't participate in healing. However, they are slowly broken down by proteases in the wound exudate. This decomposition process produces small, odorous molecules such as putrescine and cadaverine. This odor is very similar to the smell of an infection, but the difference is that the surrounding skin is not red, swollen, hot, or painful, and the patient does not show signs of systemic infection. The treatment is not antibiotics, but rather wound cleaning to remove the necrotic tissue, and the odor will naturally subside.
Another scenario is keratin breakdown caused by exudate immersion. Prolonged immersion of the skin around a wound in exudate leads to maceration, where keratin in the stratum corneum is broken down by bacterial enzymes or the wound's own proteases, producing an odor similar to ammonia or urea. This odor is different from the foul smell of an infection; it's closer to a pungent chemical smell. Treatment focuses on controlling exudate, using more absorbent dressings, and applying zinc oxide ointment or a skin protectant to the surrounding skin to reduce maceration.
Another easily overlooked issue is the dressing itself. Some occlusive dressings, if used for too long, can cause exudate to become trapped inside and develop a rancid smell, like the stale smell of clothes that haven't dried properly. This odor is produced by the natural degradation of proteins and lipids in the exudate in a warm, enclosed environment, and does not indicate an infection in the wound. The solution is simple: increase the frequency of dressing changes or switch to a more breathable dressing.
Can medications and food affect smell?
The type of topical medication can also change the smell of a wound. After using iodine-containing preparations, the wound may emit a slight iodine or metallic smell. After using silver-containing dressings, the wound may sometimes have a faint metallic smell. These smells are harmless and do not require treatment. Systemic factors should not be ignored either. Some foods, such as garlic, onions, and curry, have metabolic products that circulate throughout the body via the bloodstream, including wound exudate, giving the exudate a distinctive food odor. This condition usually disappears one to two days after stopping consumption of these foods.
How do you determine if antibiotics are needed to detect a foul odor?
A practical method of assessment is to observe the skin around the wound and the patient's overall condition. If the skin around the wound is normal in color, not hot, and without significant swelling, and the patient's body temperature is normal and mental state is good, then the odor is most likely not caused by infection, and antibiotics are not necessary immediately. Thorough debridement should be performed first, removing necrotic tissue, eschar, and fibrous membranes. Then, the wound should be rinsed with sufficient saline solution, and a new dressing should be applied. Observe for 24 to 48 hours. If the odor significantly decreases or disappears after debridement, the problem lies in the necrotic tissue; continue debridement and dressing changes. If the odor persists after debridement, and a grayish-white membrane begins to appear at the base of the wound, or the exudate becomes cloudy, then infection should be considered. A bacterial culture and drug sensitivity test should be performed on the secretions, and a sensitive antibiotic should be selected based on the results. A simple bedside test involves taking a small amount of exudate from deep within the wound with a sterile cotton swab, smearing it on a glass slide, and smelling it. Infectious odors are often very pungent and persistent, while non-infectious odors are relatively mild and dissipate quickly after debridement. However, the most reliable method is still to perform a Gram staining smear of the secretions. Seeing a large number of white blood cells engulfing bacteria under a microscope is the definitive evidence of infection; relying solely on smell is not accurate enough. For more information on Innomed® Silicone Foam Dressing, refer to the Previous Articles. If you have customized needs, you are welcome to contact us; You Wholeheartedly. At long-term medical, we transform this data by innovating and developing products that make life easier for those who need loving care.
Editor: kiki Jia


